
Intraoperative MRI enhances precision in glioma resection
FieldStrength MRI magazine
Tokai University Hospital excels with streamlined MRI-guided neurosurgical workflow
MRI is not simply an indispensable diagnostic tool, neurosurgeons can harness the modality intraoperatively to improve neurosurgical confidence and the completeness of CNS tumor resections. In clinical use for 30 years, centers can implement intraoperative MRI cost-effectively – particularly in a shared imaging equipment arrangement - as professionals at Tokai University Hospital in Japan have demonstrated.
Mitsunori Matsumae, MD, DMSc is Professor and Chair of Neurosurgery at Tokai University School of Medicine and Neurosurgeon in Chief at Tokai University Hospital. Prof. Matsumae has practiced general neurosurgery since 1988 and his primary activities in this field grew to encompass head injury management, brain tumor surgery and new imaging techniques.
A cost-effective solution
Intraoperative MRI (ioMRI) has been performed for three decades, providing neurosurgeons with up-to-date image information during neurosurgery procedures [1]. Tokai University Hospital’s (Kanagawa, Japan) neurosurgeon Prof. Mitsunori Matsumae, MD, has been performing intraoperative MRI to resect a variety of brain tumors – particularly gliomas – using his center’s sophisticated and cost-effective multi-modality imaging suite. The suite, which opened in 2006 at Tokai University Hospital and has received continuous updates since then, includes a Ingenia 1.5T MR-OR intraoperative MRI system equipped with Compressed SENSE. The multi-modality imaging suite – employed for both intraoperative MRI procedures and diagnostic imaging in a shared arrangement – has been acost-effective solution for Tokai University Hospital, which has become a leading facility in interventional radiology and image-guided surgery.

Increasing the potential of gross total tumor resection with intraoperative MRI
“Generally, the outcome of glioma surgery is strongly related to how much of the tumor is resected [2-3],” Prof. Matsumae says. “Because glioma is an infiltrative disease, it is important to remove as much tumor as possible, while also preserving neurological function. Thus, surgical planning by carefully observing the relationship between the glioma infiltration area and eloquent region is needed. ”With its undisputed soft tissue visualization, MRI is the modality of choice for diagnostic (pre-operative), intraoperative and post-operative imaging.
“Intraoperative MRI is needed because MRI is the clinical gold standard for identifying the lesion and evaluating the extent of resection with both preoperative and post-operative images,” he observes. “Neurosurgeons acquire intraoperative MR images to characterize the surgical procedure performed and to consider whether the surgical strategy needs to be revised for the next step.”
Key advantages of intraoperative MRI
Prof. Matsumae summarizes four key advantages of intraoperative MRI during a glioma resection procedure:
After the initial craniotomy, intracranial pressure increases, causing the brain to bulge. In addition, the brain shifts in various directions during resection due to aspiration of cerebrospinal fluid, expansion of the compressed brain, and increasing brain edema. This brain shift increases as surgery progresses, and, consequently, the accuracy of neuronavigation based onpreoperative MR images decreases. Neurosurgeons, therefore, want to use intraoperative MRI to update and re-register images for neuronavigation as surgery continues.
Intraoperative MR images can reveal unexpected tumor remnants.
Evaluation of surgical success: When the neurosurgeon has determined that the glioma has been removed to some extent, it is not only the percentage of the lesion resected that is important to as certain, but also the relationship between the remnant tumor and eloquent regions, connecting fibers, ventricular wall and major vessels. The latter can inform the degree of risk involved in continuing the resection.
Intraoperative MR images can be used for early detection of unexpected vascular complications.
Generally, the outcome of glioma surgery is strongly related to how much of the tumor is resected.”
Prof. Matsumae, MD
Equipment sharing makes intraoperative MRI economically feasible at Tokai University Hospital
In Prof. Matsumae’s view, neurosurgeons value intraoperative MRI as a tool to improve surgical results, but this desire does not supersede financial considerations. At Tokai University Hospital the Ingenia MR-OR is part of a sophisticated MR/CT/angiography/operating room (MRXO) suite that permits efficient image-guided neurosurgeries. “The bottleneck for introducing intraoperative MRI is the initial cost,” he says. “Installing an expensive MRI system within an operating room is disadvantageous in terms of cost effectiveness, so sharing the equipment can be a practical solution. At our hospital, the imaging systems are located close to each other, separated by shielded doors. In this multi-theater setup, each system can be used independently or in different combination. Therefore, the Ingenia MR-OR can be employed for intraoperative MRI, and when not in combined use the MRI can be separated and used for routine diagnostic imaging to maximize cost performance via high throughput.” High throughput is virtually a guarantee at Tokai, as the MRXO suite is adjacent to, and part of, the emergency department. Therefore, the imaging systems can be operated 24 hours a day, 365 days a year.

Layout of the intraoperative MRI suite as part of the MXRO suite. The OR-angiography room is located in the middle and the MR imaging and CT units are situated in rooms on either side. The Ingenia 1.5T, operating table, angiography bay and CT unit are in an in-line orientation, which facilitates the patient’s smooth transport from table to table. The MR and OR room are connected by RF-shielded doors. Using a fully MR-compatible IntraOP transfertrolley (Mizuho Co.), the patient is transferred from the OR table to the MR, while positioned on a transfer board throughout patient transport and imaging.
Focus on MR safety minimizes risks and enables fast procedures
Tokai staffing for a glioma resection surgery includes one or more neurosurgeons, circulating nurse, scrub nurse, neuromonitoring technician (i.e., for motor-evoked and somatosensory-evoked potentials), anesthesiologist and medical residents. An intraoperative MRI procedure adds an MR technologist, radiologist and a nurse safety manager, the latter appointed to oversee safety and strictly manages (via a read-aloud checklist) key steps during patient transfer between the Ingenia system and operating table. “In intraoperative MRI procedures, the standard workflow is altered to when the patient is moved to the MRI,” Prof. Matsumae says.“All involved staff participate in multi-disciplinary discussions and simulations to standardize the processes. MR safety is the keyword in the intraoperative workflow to minimize risks and enable procedural efficiency.”
Neuronavigation system provides effective roadmap for surgery
Patient preparation is the same for intraoperative MRI operations and procedures that won’t involve interoperative MRI. Tokai University employs a Brainlab neuronavigation system with automatic image registration. This system references the brain (Cartesian) coordinate system with a parallel coordinate system of the patient’s pre-operative 3D MRI image data. Neuronavigation provides intraoperative orientation to the surgeon, helps plan a precise surgical approach to the targeted lesion, and defines neurovascular structures. During surgery, Prof. Matsumae consults the neuronavigation display periodically to determine if the navigation parameters (i.e., surgical trajectory to tumor) are still accurate.
If I notice that the navigation is out of position due to brain shift or brain bulging, intraoperative MRI will be used to update or correct it.”
Prof. Matsumae, MD
Efficient workflow streamlines acquisition of MR images
An observed out-of-position neuronavigation will prompt the surgical team to prepare for intraoperative MRI [4-5]. Under the direction of the nurse safety manager, all ferromagnetic instruments are removed from the surgical field and the surgical wound is covered with a sterile drape. These preparations take about 10 minutes, followed by an in-line patient transport to the MR-OR using a Mizuho IntraOP transfer trolley. The anesthesia machine and monitors are transported together with the patient to the MRI unit. “Prior to the patient transfer, the MR technologist can prepare the Ingenia MRI from diagnostic use to intraoperative use in as little as two minutes and we can move the patient from the OR to the MRI room in one fast procedure,” Prof. Matsumae notes.

Ingenia MR-OR 1.5T installation with short, in-line transfer between OR and MR suite using Mizuho IntraOP transfer trolley and NORAS OR Head Coil.
Short scan times, detailed image information
To enable evaluation of resection completeness or to acquire images to correct for brain shift, the MR staff will perform several sequences using a NORAS OR head coil (see Tokai ExamCard Table). Standard protocols for high-grade gliomas include:
| Sequence | Benefit | Resolution, C-SENSE factor, Typical scan time |
| Marker 3D T1W TFE | Marker visualization | 1.56 x 1.64 x 5 mm C-SENSE factor 3 0:31 min |
| 3D T1W TFE without and with gadolinium (Gd) enhancement | Contrast-enhanced T1 is useful because high grade gliomas are typically Gd-enhanced. | 1.03 x 1.08 x 1.20 mm C-SENSE factor 3.5 1:47 |
| 3D FLAIR BrainView | For non-enhancing gliomas. Helps in identifying low-grade glioma and for distinguishing brain edema from tumor. | 1.1 x 1.1 x 2.4 mm C-SENSE factor 5 5:01 min |
| Diffusion tensor imaging (DTI) | Visualization of the anatomical location of white matter tracts. Fiber tracking software converts these images to a parametric color-coded display of white matter fiber tracts. In tumor resection surgery, it is critical to know the topographic relation of white matter fiber tracts (e.g., associated with Broca’s or Wernicke’s functional areas) that are near a lesion and the connecting fibers originating from these regions. | 3 mm isotropic 3:14 min |
| Diffusion-weighted (DWI) | Evaluation of ischemic complications (e.g., stroke). | 1.9 x 1.9 x 5.0 mm 0:45 min |
Because imaging speed in intraoperative MRI is important at Tokai, the center has been using SENSE parallel imaging since the beginning. In 2020, the team started employing Compressed SENSE instead to achieve greater scan time reductions. “At our hospital we prioritize speed and we have seen that Compressed SENSE helps us to reduce intraoperative MRI scan
time for our 3D T1W scans with about 40%.” Dr. Matsumae says.
Shorter scan time in intraoperative scans
Compressed SENSE reduces scan time from 3:59 min to 2:55 min with the same spatial resolution.


Using up-to-date MRI information for enhanced confidence
The intraoperative MRI scans are evaluated and can be used to update neuronavigation, guide the surgeon on the location of tumor remnants that can be further resected, or inform the decision to forego further tumor resection to preserve neurological function. “Regarding the last point, ambitious surgical invasion in an attempt to resect the entire lesion can cause serious neurological dysfunction,” he explains. “So, neurosurgeons may decide to not ‘chase’ the lesion deeper and rather continue treating the remnant with chemotherapy or radiation therapy.” Restarting a resection procedure after an intraoperative MRI scan takes about 10 minutes; the total time used for intraoperative MRI cases averages 30 minutes including preparations, patient transfer, image acquisition and restart. A post-operative MRI scan is done immediately after resection when the neurosurgeon suspects is chemic complications based onthe intraoperative MRI DWI images. However, typically the post-op MRI – in the Ingenia MR-OR or at one of Tokai’s other six Philips MRI systems – is performed the following day absent complications.
The Brainlab neuronavigation system employs automatic detection of MR marker spheres, which are attached to the NORAS head coil to update anatomical data during the operation. In this way, physicians can efficiently assess brain shift or evaluate resection progress.
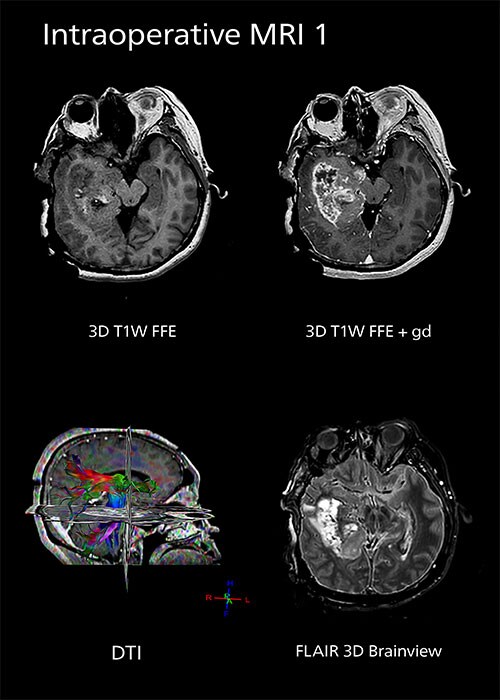
Clinical case: Intraoperative MRI to update neuronavigation
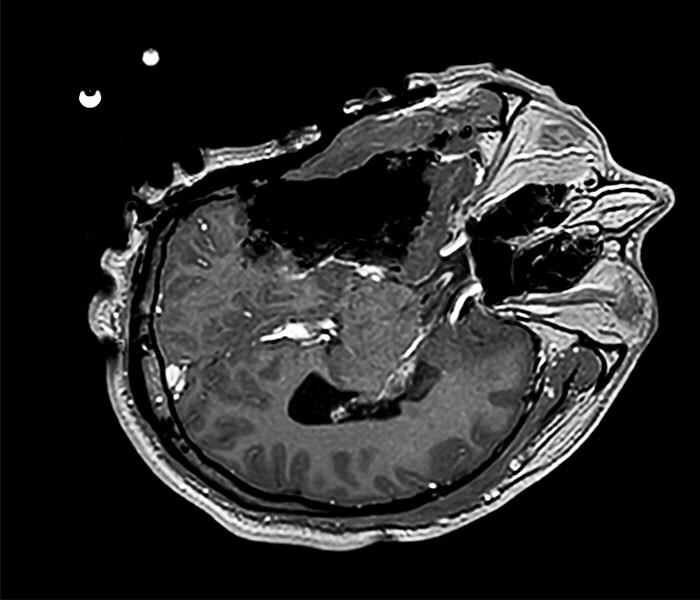
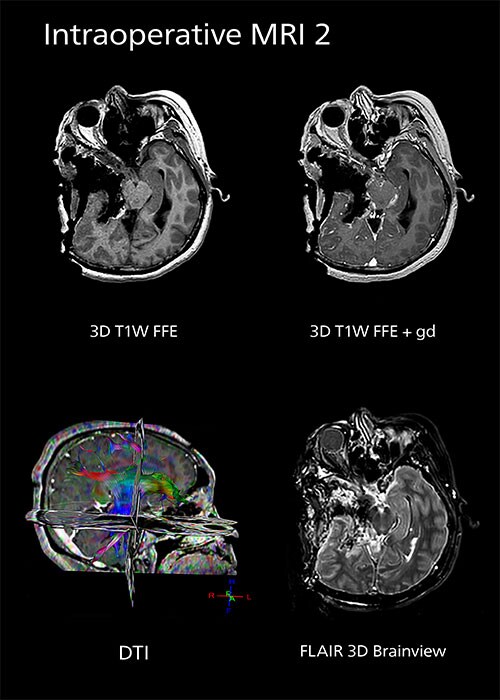
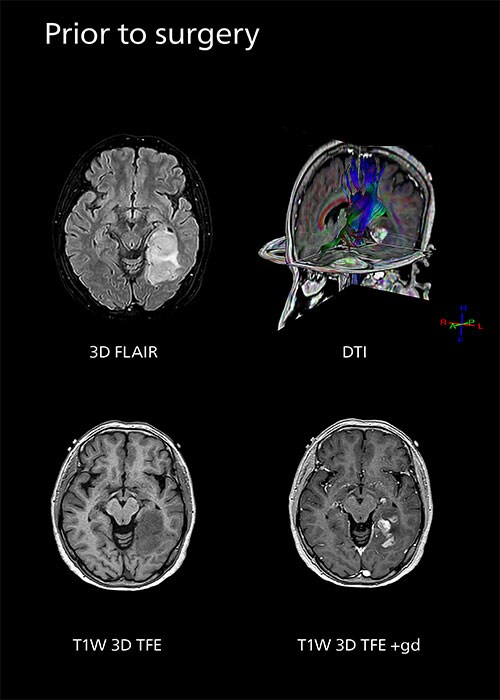
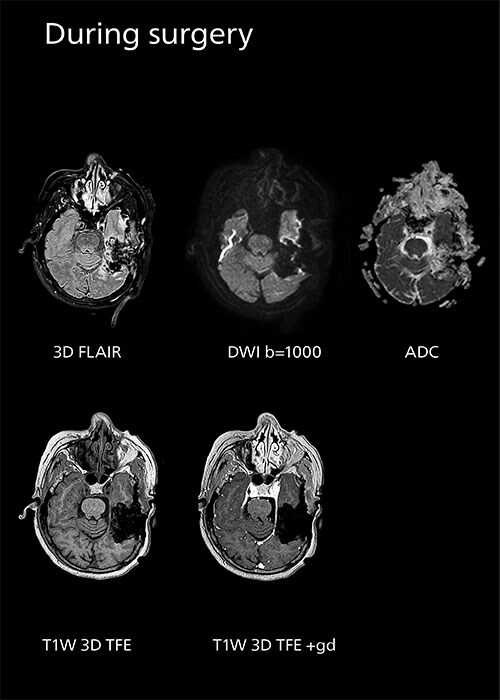
In a patient experiencing headache, the pre-operative MRI showed a high-grade glioma in the right temporal lobe. The first intraoperative MRI scan was used to update neuronavigation to compensate for brain shift, the second intraoperative MRI scan showed satisfactory resection of the lesion.
Clinical case: Intraoperative MRI confirms complete tumor resection
A patient first experienced epilepsy. The diagnostic MRI showed brain tumor in the left temporal lobe. On the day of surgery, pre-operative images were acquired. Surgery was performed in the MR-OR suite, and the intra-operative MRI showed satisfactory removal of the high-grade tumor.
Clinical case: Intraoperative MRI guide surgical decision making
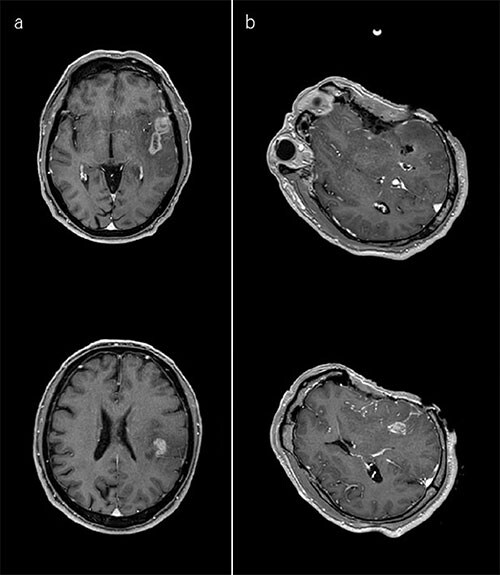
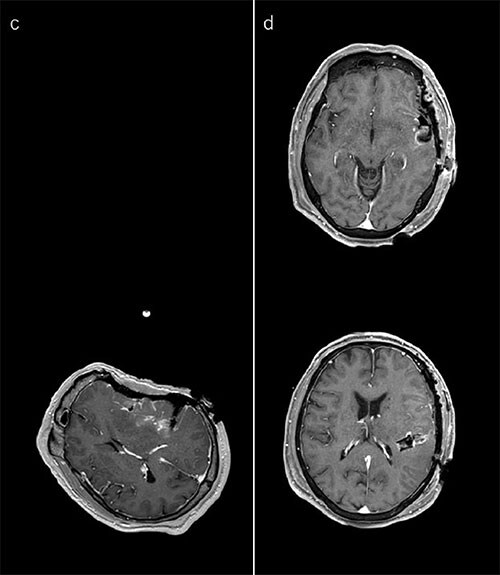
A patient presented with skipped lesions (a). The first intraoperative image confirms resection of the anterior part of the tumor. At that time, the surgeon found it difficult to reach the posterior part because the microscope light did not project the surgical corridor. Accordingly, it was decided to change to another corridor based on the result of the first intraoperative MRI image. The register images for neuronavigation were updated (b). The second intraoperative image shows tumor remnant at the anterior part of thecorridor. The register images for neuronavigation were updated (c). The day after surgery, post-operative images show a satisfactory surgical result (d).
Intraoperative MRI feedback boosts neurosurgical skills
“Intraoperative MRI provides the feedback needed to differentiate tumor versus eloquent structures or simple edema,” he says. “This feedback also sharpens the neurosurgeon’s skills over time, such that the number of MRI scans needed during a surgical procedure decreases.”

Since Prof. Matsumae began using intraoperative MRI, he has found that his skill in achieving gross tumor resection in glioma resection has increased, a reflection of the quality of feedback he is receiving from the intraoperative MRI scans. “In the early years, resection completeness ranged from 50 to 60 percent, even with four to five intraoperative MRI scans persurgery,” he notes. “Today, in about 70 percent of cases, the initial resection is considered a satisfactory tumor resection [≥ 98 percent resected]. ”In the cases where intraoperative MRI is used, it’s seldom more than one scan. The decision to perform a second intraoperative MRI scan is determined by “the surgeon’s proficiency, intraoperative impression and surgical plan,” he says. Prof. Matsumae attributes his center’s increasing success rates to periodic upgrades of its Philips MRI hardware and software that have enhanced image quality and shortened acquisition time, as well as the insights on anatomy and pathology provided bythe intraoperative MRI procedure itself.
References
Results from case studies are not predictive of results in other cases. Results in other cases may vary.